In This Corner
My Brush with Lou Gehrig’s Ghost
Some unfamiliar sensations led this doctor to start worrying—and have more empathy for his patients

Mission to Haiti
A member of the first U.S. medical team to respond after the earthquake reflects on working in a disaster zone
By Leslie Macmillan
On January 18, six days after a 7.0 magnitude earthquake devastated Haiti, a Massachusetts medical team was the first from the United States to treat patients there.
Geoff Bartlett, a staff member in Tufts’ department of public and environmental safety, was a logistics expert on the team. He has been with the group for 10 years, and served on medical missions after September 11, Hurricane Katrina and an earthquake in Iran. His main responsibilities are logistical—he sets up the satellite and radio contact with the outside world as well as the medical records system—and because he is a trained EMT, he helps care for patients, too.

Geoff Bartlett, left, with other members of the medical assistance team in Haiti in mid-January. Photo: Joseph Conlon
The Massachusetts-1 Disaster Medical Assistance Team arrived at its staging site—a university courtyard—at 10:30 the night of the 17th, and by 7 a.m. had set up a mobile hospital in the midst of a tent-city displacement camp. In one week, the team saw 505 patients, performed 66 surgeries and delivered nine babies.
Tufts Journal: What was a day like for the team?
Geoff Bartlett: We worked 12- to 16-hour days, and we saw patients day and night. The Army ambulances would come in two at a time. When they pulled up, you knew you had at least eight patients on stretchers. I saw more orthopedic injuries than I’d ever seen in my life. Gruesome fractures. There were wound infections the likes of which I’d never seen. They just didn’t have the ability to keep them clean. There’s no appropriate way to describe the way some of these wounds smelled. There were injuries that, because they had become infected and because of the resources that were available for care afterwards, the only course of action was to cut the limb off.
That’s a very difficult decision for a medical provider to make because in that environment, a limb amputation could be a death sentence. Haitians don’t have a lot of opportunities for work that don’t necessitate being physically able. At the same time, if we fail to stop the infection, that would be a death sentence, too.
You couldn’t have brought all the medical supplies necessary—did you have to improvise?
We had a lot of kids who came to us without any kind of parents or family. We had to make do with the supplies we had available. An infant we named Katie from Haiti needed an incubator—that’s what would be used in an intensive care unit in the United States. But we don’t carry an incubator with us, so we made one out of heat-reflective blankets. During the day, it was pretty warm out, but at nighttime, if things got too cool, we would take turns holding her. We were all hot from working all day, so that’s how we kept her warm.

The tent city outside of the improvised hospital where the U.S. medical team worked. Photo: Joshua Kelsey, U.S. Navy
What was hardest about your work in Haiti?
One of the really tough things for those of us who are there to support the medical mission is walking by all these people in desperate need, and you feel this sense of guilt that you have to stay focused on what your job is.
Once I finished my shift, I’d see what I could do to help out in the tents. One night I walked into the ICU and saw this two-year-old playing on the floor, his leg all wrapped up in an Ace bandage that stopped right below the knee. He had recovered from anesthesia and they were trying to keep him entertained there. One of the extra pieces of equipment we bring is a duffel bag of stuffed toys so that we can help kids still be kids. He didn’t understand what had happened, probably didn’t even appreciate that his own body was different, but it was shocking to walk in and see.
Another day I saw a girl with a thigh bone fracture, before her surgery, just crying inconsolably. She was probably 9 or 10 years old. She didn’t lose her leg, but we needed to fix the fracture. In the U.S., if you were under long-term orthopedic care, they might do that with pins or a plate, but the standard of disaster medicine is to use a device called an external fixator. You have rods that screw into the bone, but they extend outside the skin, and there’s a steel scaffolding that can connect to these rods, and it keeps the bones very rigidly fixed and aligned.
I was in the ICU helping out again when this girl was in recovery, and she was just waking up and hadn’t seen what was going on yet. I was there when she first sat up and looked at her leg. Now, imagine she’d probably never had any exposure to what Western medical care is like, maybe had never seen a doctor in her life. She woke up and here are all these people speaking a language she doesn’t understand, who had done something to her that she doesn’t understand, and there’s this metal scaffolding sticking out of her leg. She lets out this howl you could hear across the camp. We’re trying to calm her down, trying to get a translator over to explain this is going to help your leg heal, that it’s not permanent. Imagine what a 10-year-old girl thinks when you’ve just done that to her body, because at that age, they are very self-aware.
Did you care for orphans, too?
There was one kid about two or three years old we called Popeye—we never did find out what his real name was—who came in with a broken arm. We could have turfed him off on the orphanage a little sooner, I suppose. But Popeye grew on us, because if he wasn’t being held, he would just cry inconsolably. And that doesn’t contribute to peace in the camp—especially since we were trying to keep other kids happy, too. Crying is contagious. So anyone who didn’t have their hands full would hold Popeye. I would hold Popeye for a couple hours in the command post while we had our staff meeting. He’s asleep in my arms, and we’re all going about business, but it kept the peace.
We were convinced Popeye was going to be an orphan. But on the day that we were leaving, we were at the airport and got word from the replacement medical team that his mother had shown up at camp and there was a reunion.
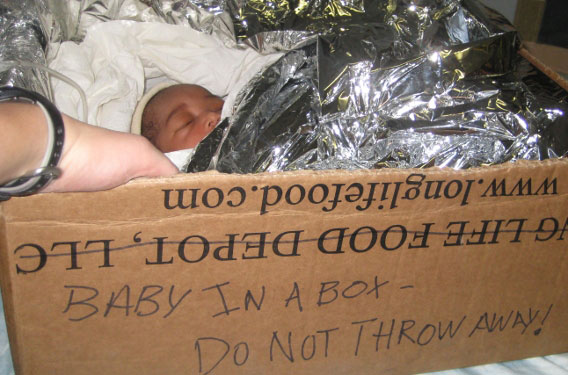
An improvised incubator for the infant the team nicknamed Katie. Photo: Jennifer Lewis
What was the reaction of the Haitians to the disaster?
Every morning when we got up, and every evening when the sun went down, people in the tent city next to us were singing. We were told the rough translation is they were singing their thanks and praise to God for having seen them through the earthquake still alive, and thanks for what they did have left.
Did seeing the disaster up close take a toll on you and the team?
When you’re working long days, you don’t have time to think about these things, and you sleep the sound sleep of a day’s hard work. It’s when you leave that you start to process.
Actually, the worst night’s sleep I got there was the last night we were in-country. We were sleeping in the same type of tent we’d been working in, and a few times in the night I woke up thinking I was in the middle of a tent full of patients. I’d wake up from dreaming about moving litters around, seeing more ambulances carrying more patients.
How would you sum up the experience?
We’re very proud of the fact that we were first on the ground and that we built that hospital. We think we accomplished a lot. But we knew it was an unfinished job.
Immediately after we got back to the States, we devised a roster of who of us could re-deploy. It’s unlikely we will—in Haiti, they’re transitioning to long-term aid now and that’s not our function—but I’m on the list. If they send the team back, I’m ready.
Leslie Macmillan can be reached at leslie.macmillan@tufts.edu.